
Delaware treats health data like a road system 🛣️, Agents don't get a pass 🪪

***Note: The original post mentioned Medgemma release, which is “old news.“ Interesting how my AI curation let that slip through as it was released almost one year ago to the day*****

⚡ Around the Wards
Delaware turned health-data exchange into a public utility — real-time insurance eligibility and prior auth now run through one neutral statewide hub (built on the state HIE, DHIN) instead of forty portals and a fax machine, and on July 13 the governor stood up the state’s first Surgeon General to drive the policy. 🔮 My bet: three more states copy the “neutral hub as public infrastructure” model within 18 months — and the vendors who sold point-to-point integrations spend 2027 explaining why anyone still needs them.
Octozi raised $3M to put agentic AI on clinical-trial data cleaning — a published study reports reviewer error rates falling from ~54.7% to 8.5% with a human-in-the-loop grader. The number that matters isn’t the funding; it’s the error curve.
🎧 Podcast: The 229 Podcast — “Agents Don’t Get a Pass: Governing Digital Identity” — AI agents are now one of the fastest-growing identity types in a health system, and if an agent improperly discloses PHI, “OCR won’t care whether it was a person or a machine. You’ll still be accountable.”
🧭 The Curbside
“Should our AI agent get its own login to the EHR?”
Short answer: Only if you can answer “what’s the blast radius?” before you provision it.
What changed / Evidence: The identity problem is now the governance problem. As one healthcare security leader put it this week, agents are becoming one of the fastest-growing identity types in the hospital, and accountability for what they access and disclose lands on you regardless of whether a human or a machine did it.
Builder read / Watchout: Give the agent the least access that lets it do the job, scope it to specific resources, and log every action to something a human reviews. 😤 Haters: “This is just IAM with extra steps.” Kind of — except the agent acts continuously, at machine speed, on data with a federal penalty attached. The extra steps are the point.
🔬 The Big Thing
What if the health-data hub isn’t a product to sell — but a road the state paves? Delaware just tested the idea.
Delaware routed real-time insurance eligibility and prior authorization through a single neutral statewide hub, built on the state’s health information exchange (DHIN) and the Smart Health Network — connecting clinicians, payers, and health systems to one shared pipe instead of forty portals and a fax machine.
The same week, on July 13, Governor Matt Meyer signed an executive order creating Delaware’s first Office of the Surgeon General and named otolaryngologist Dr. Neil Hockstein — who chairs the state Health Care Commission — to the role.
The move that should stop a builder cold: Delaware treated interoperability as public infrastructure — “neutral, and designed around patient interest” — not as a market to be won by whichever vendor sells the most integrations.
Healthcare runs on an estimated nine billion faxes a year because every organization built its own private connection to every other one — “a different dirt road for every different type of car to everywhere else.” A neutral hub says: connect once, reach everyone. That’s a structurally different bet than another point-to-point product.
If you build eligibility, prior-auth, or data-exchange tooling, this is the question the next 18 months will ask you: are you paving the public road, building the on-ramps to it, or selling one more private dirt track that a state utility just made redundant?
😤 “It’s Delaware. A million people. This doesn’t generalize.” Small is the feature, not the bug — it’s big enough to matter and small enough to actually ship. The first state utility always looks like a rounding error. Then it’s the template three neighbors copy because building your own from scratch is dumber than joining one that works.
😤 “State-run health infrastructure? That’ll move at DMV speed and vendors will route around it.” Maybe. But it’s built on DHIN — a HIE that’s been live for years — not a greenfield IT project. And “neutral utility” is exactly the thing no single vendor could ever credibly be, because every vendor’s incentive is to own the pipe, not share it.
😤 “Prior auth is a fight AI won’t win — a hub doesn’t change the denial.” Right, and the hub isn’t trying to win the fight. It’s trying to make the plumbing invisible so the fight is faster and the patient can see the tracker. Different problem. Both real.
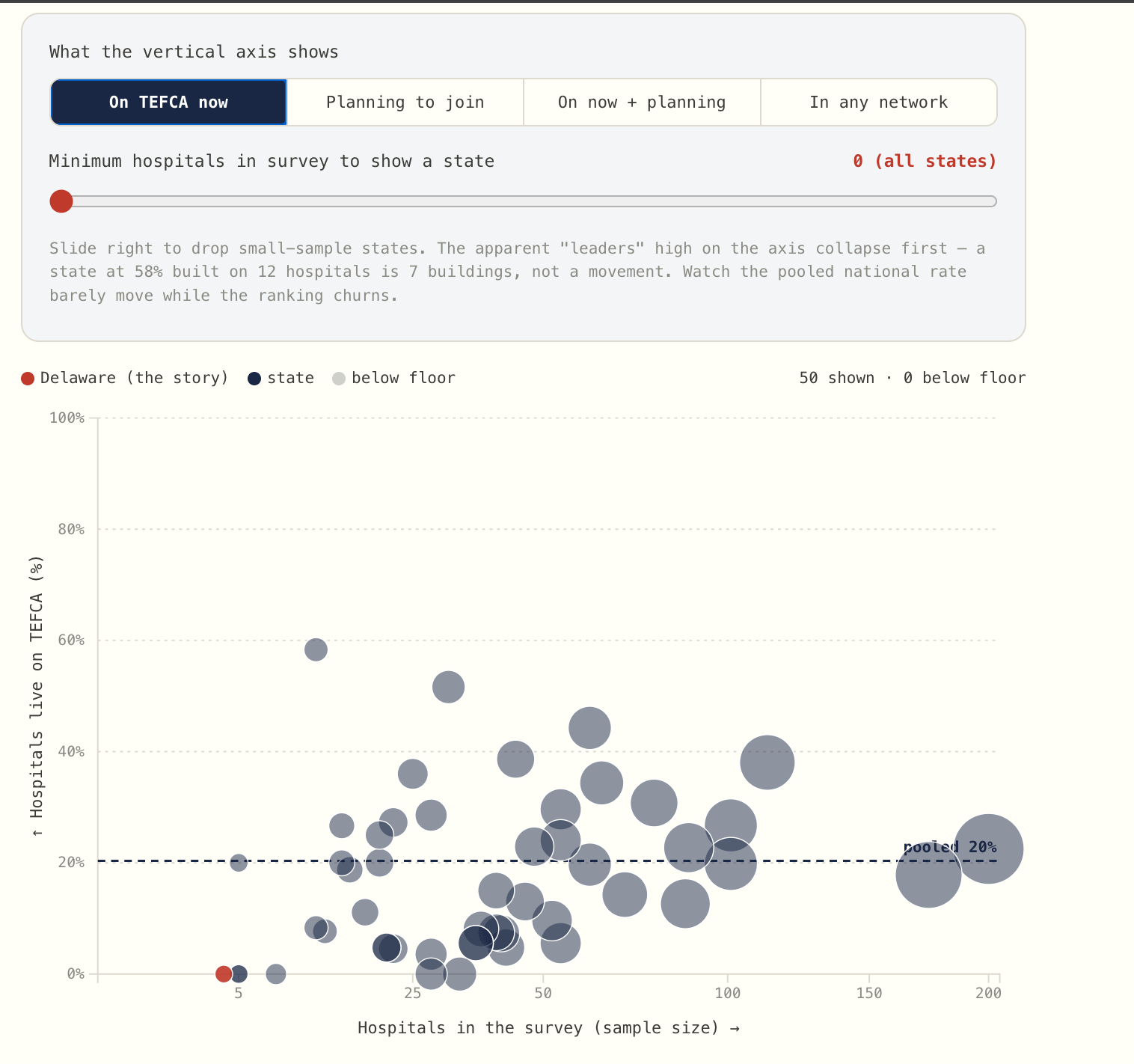
🧪 Try the interactive: The Public Road — all 50 states plotted by how many hospitals are on the “connect once, reach everyone” road vs. still just planning. Built with real CMS data via mimilabs.
📡 Builder’s Radar
The number that should reset your priors on “AI for paperwork”: 54.7% to 8.5%.
Octozi raised a $3M seed (Surface Ventures, Remarkable Ventures, Debiopharm’s venture arm) to put agentic AI on clinical-trial data operations — the cleaning, reconciliation, and reporting that gate a database lock.
In a controlled, published study, their human-in-the-loop system pushed data-cleaning throughput ~6x, cut reviewer error rates from about 54.7% to 8.5%, and dropped false-positive queries roughly 15-fold — an estimated $5M+ saved on a representative Phase III oncology trial.
The story isn’t the agent. It’s that they measured the human baseline (a 54.7% error rate!) and proved the delta. Most clinical-AI pitches show you the model’s accuracy and never tell you what the humans were doing before.
😤 “Trial data ops isn’t clinical AI, it’s back-office.” The back office is where the defensible AI businesses are hiding — measurable task, human-in-the-loop, and a baseline bad enough that a real delta is easy to prove.
Vidith Phillips, MD, MS (Imaging AI researcher, St. Jude) — posted a running list of healthcare-AI GitHub repos worth knowing (awesome-healthcare-ai, awesome-healthcare, and more), a decent weekend map if you’re looking for open-source clinical tooling to learn from.
🎙️ From the Pods
🎙️ Lifers with Christina Farr — “Healthcare sends 9 billion faxes a year. Delaware has a better idea.”
The most underrated voice in the episode wasn’t the CEO or the surgeon — it was Aretha, a surgery scheduler, describing a morning spent logging into “multiple portals,” chasing prior auths that sit pending for days, only to sometimes learn no auth was required at all. That’s the user your tool is actually for.
🔇 Speaker Blindspot: Availability heuristic — the panel generalizes from Delaware’s genuinely favorable conditions (tiny, one dominant HIE) to “this is the model,” while skating past why forty other states with fragmented HIEs and no neutral convener haven’t done it. The template is real; the transplant is harder than the enthusiasm suggests.
💡 BTW
💡 BTW: Paul Meyer — the CEO running Delaware’s new neutral health-data hub — built Text4baby about fifteen years ago: a free service that texted evidence-based pregnancy and infant-health tips to millions of moms, and got so universal the team joked the only organizations not partnered with it were “those that hate babies.” Before health tech, he was a speechwriter in the Clinton White House. Same idea running through all of it: build the thing for the person, and every institution finds its own reason to show up.
What are you building this week? Email and tell me (kevin@clinicians.build) — I read every one.
— Kevin & AI