
Congress votes on prior auth twice 🏛️, MDCalc grades the calculators 📊, Lilly buys into the ring 💍


⚡ Around the Wards
Congress voted on prior auth twice this week — and took both sides on AI — Ways & Means advanced electronic-PA reform 42-0 while the Senate rejected, 46-50, a bid to halt CMS’s WISeR AI pilot. The full story below.
😤 Haters: “Bills aren’t laws.” True — but 42-0 out of Ways & Means isn’t a bill problem, it’s a countdown clock.
MDCalc started grading its own calculators — quality ratings for 800+ clinical tools, including explicit bias flags. The app in your pocket just became a referee.
Eli Lilly took an equity stake in Oura — molecule, sensor, prescriber, and data are converging under one cap table.
The AMA is building SNOMED CT–to–CPT mappings — unglamorous terminology plumbing for the January 2027 electronic-PA deadline.
🎧 Podcast: Lifers with Christina Farr — Amit Phull (Doximity) — Phull argues clinical AI is entering its “benchmarking era” and nobody has defined healthcare’s equivalent of the 190 million miles that earned self-driving cars public trust.
🧭 The Curbside
“Kimi K3 just topped the code arenas and it’s a fifth the price. Should I move my clinical side project to it?”
Short answer: Try it for code. Don’t trust it for clinical reasoning yet.
What changed: Moonshot released Kimi K3 this week — 2.8T-parameter MoE, 1M-token context, roughly $5.40 blended per million tokens versus ~$9–10 for the US frontier, and #1 in the Frontend Code Arena. Open weights are promised for July 27 — announced, not shipped.
Builder read / Watchout: The number that matters for us went the wrong way: hallucination rate rose to 51% from 39% in the prior version, even as accuracy improved. Cheap and confident is a dangerous combination at the bedside.
❓: Some are saying it is cheaper per token but takes more tokens to accomplish a task, making the cost comparable to Sol.
“Our patient-access app runs on Azure API for FHIR — what actually breaks this fall?”
Short answer: Your auth breaks before your data does.
What changed: Azure API for FHIR retires September 30, and the SMART on FHIR proxy retires September 21 — that’s roughly ten weeks. The replacement Enhanced flow in Azure Health Data Services is a re-authorization architecture, not a config toggle.
Builder read / Watchout: Sequence the auth migration first: inventory your SMART scopes, re-test launch context under SMART v2, and run a parallel staging environment before cutover. Treat it as a security-review ticket, not an infrastructure chore.
🔬 The Big Thing
Congress voted on prior auth twice this week — and took both sides on AI.
On Tuesday and Wednesday, House Ways & Means advanced the Improving Seniors’ Timely Access to Care Act 42-0 — mandatory electronic prior auth for Medicare Advantage, time-bound decisions, HHS oversight.
The same markup advanced an MLR Transparency Act 42-0, forcing MA plans to disclose how much revenue actually goes to patient care. And Reps. Greg Murphy and Herb Conaway introduced the bipartisan Protecting Patients from Automated Denials Act, aimed squarely at AI-driven denials in MA — months after West Virginia rewrote its own prior-auth law after a patient died waiting.
Then the Senate rejected — 46-50, party line, White House lobbying — a bid to halt CMS’s own WISeR AI prior-auth pilot in traditional Medicare.
So in one week: Congress moved to restrain denials in Medicare Advantage and voted to protect an AI denial pilot in fee-for-service. The tension isn’t between government and industry. It’s inside the government.
The signal isn’t pro-AI or anti-AI. It’s that the appeal, not the submission, is where the leverage lives.
Look at the KFF post-acute data everyone in that hearing room was holding: MA plans deny 65% of long-term-care-hospital and 54% of inpatient-rehab PA requests. Of SNF denials that get appealed, 95% are overturned.
Only 18% are appealed.
That’s four out of five improperly denied stays where nobody ever said “check again.” The voluntary insurer-pledge era is ending; the legislative era is starting. Either way, the appeal gap is the fight a builder can actually win.
😤 “These bills die in the Senate like every doc-fix before them.” Maybe. But transparency provisions have a way of outliving their parent bills — and 42-0 means payer transparency is now a bipartisan sport. The disclosure requirement is the part I’d bet survives.
😤 “Payers will just relabel AI denial as ‘augmented human review.’” That’s exactly why the Murphy-Conaway bill matters — it targets the function, not the label. Watch the definitions section, not the press release.
😤 “You’re reading a lot into one procedural Senate vote.” Read the whip count then. 46-50, party line, with the White House lobbying to keep an AI denial pilot alive. That’s not procedure. That’s a position.
❓ If MLR disclosure passes, someone gets to build the Bloomberg terminal of the denial economy — plan-level denial and overturn benchmarks, priced per seat. Who should own that dataset: an RCM vendor, a transparency startup, or a neutral third party? I keep going back and forth.
🧪 Try the interactives: Two ways into today’s Big Thing, built with real CMS data.
A — The Appeal Nobody Files — Watch 100 SNF denials play out: 95% of appealed denials are overturned, only 18% are ever appealed — and see the four out of five wrongly denied stays where nobody ever said “check again.”
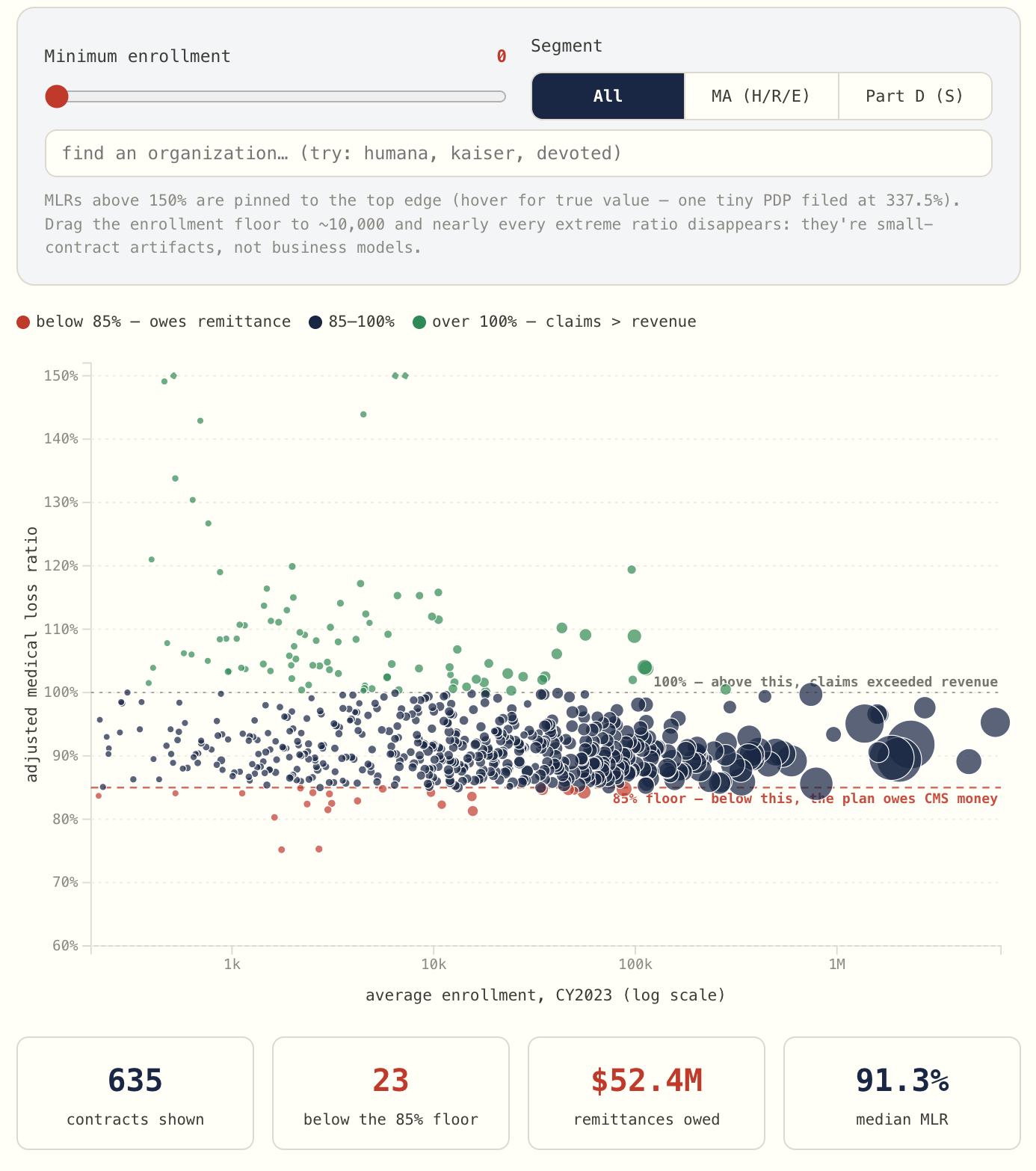
B — The Denial Economy’s Public Ledger — The ledger the MLR Transparency Act wants to open already has a public v0: every Medicare Advantage and Part D contract’s 2023 medical loss ratio filing — 635 contracts, one dot each, $537.8B in revenue.
📡 Builder’s Radar
The calculator app more than half of US physicians open every month just started grading its own tools.
MDCalc launched a Quality Rating System for its 800+ clinical calculators — rating importance, scientific soundness, fairness and equity, and usability, with explicit flags for algorithmic bias and population-level harm.
Co-founder Joe Habboushe, MD and Dr. Shazia Siddique built the criteria by Delphi consensus with an advisory board — the same tool clinicians already trust, now telling you which of its own instruments are poorly validated.
A distribution platform turning itself into a referee is a bigger deal than any single AI model release.
😤 “A store grading its own inventory — how convenient.” Then steal the move. The methodology is published, the criteria are public, and the incumbent risked its own catalog to do it. Name another clinical AI vendor that flags its own weak products.
Eli Lilly took an equity stake in Oura — the third move in seven weeks.
First the LillyDirect partnership, then in-app GLP-1 Insights, now ownership. Molecule → sensor → prescriber → data, one entity holding the chain. WHOOP, meanwhile, just had a wrist-glucose patent application published.
When the drugmaker owns the sensor measuring its drug’s response, the sensor’s API is no longer a neutral utility.
🔮 My bet: Within 18 months every GLP-1 maker owns or leases a wearable, and the independent wrist-to-chart bridge — the layer that doesn’t answer to pharma — becomes a fundable product category.
The Patients First Act is hiding a PMPM primary care pilot — the first time Congress has proposed paying Medicare PCPs the way DPC practices charge.
Buried in the physician-pay bill introduced Wednesday: a five-year Medicare pilot paying a per-member-per-month fee on top of fee-for-service.
That creates a software category that doesn’t exist: Medicare-eligible PMPM panel management for independent PCPs who aren’t in an ACO. The ACO platforms are too heavy for them; the DPC platforms only serve the cash market.
💡 80/20: If this pilot survives markup, the first buildable piece is beneficiary attribution and reconciliation against CMS data — the boring FHIR service every PMPM tool will need and none of the incumbents ships for the middle market.
OpenEvidence and Boston Children’s launched a multi-year study of how point-of-care AI actually changes care — anonymous usage patterns from the EHR, correlated with care delivery.
⁉️ A vendor underwriting a multi-year study of its own tool’s effect on real care patterns — the anonymized exhaust becomes the evidence engine. I’m genuinely unsure whether that’s the validation infrastructure we’ve been asking for or marketing with an IRB number. Watching this one.
The AMA convened a SNOMED CT–to–CPT mapping initiative ahead of the January 1, 2027 FHIR electronic-PA deadline. Terminology crosswalks are the least glamorous and most load-bearing part of the prior-auth stack — if your tool translates clinical documentation into billing language, this mapping becomes your substrate.
Ultra-shorts:
Samsung softened its health-data ultimatum — after an in-app notice tied cloud sync to AI-training consent and threatened deletion of synced data, Samsung now says withdrawing consent deletes only the AI-development data. The single consent still spans menstrual, medication, and medical-record data. HIPAA doesn’t reach consumer manufacturers. Nuff said.
Vital Signals opened preorders on a $399 cuffless BP ring — continuous, calibration-free, ships October. Worth knowing: AHA/ACC guidance — reiterated in a December scientific statement — still recommends against cuffless BP devices for diagnosis or management, and the FDA-grade version is “planned,” not cleared.
ICE shared improperly obtained Medicaid data with Palantir, per new court filings from 20 state AGs — including data on US citizens. Patient data trust is now a two-front problem: consumer apps on one side, government custodians on the other.
Chris Altchek (CEO, Cadence) posted a video response to the proposed Medicare RPM changes — agreeing CMS is right to target low-quality RPM while arguing for cost accountability and clinical integration over a vendor ban.
🎙️ From the Pods
Dr. Amit Phull (EM physician, Doximity’s chief clinical experience officer) argues clinical AI is entering its “benchmarking era” — and admits nobody has defined healthcare’s version of the ~190 million autonomous miles that earned self-driving cars their trust.
“Move fast, but don’t spill your drink.” — Amit Phull
💡 Builder take: Farr’s counterpunch is the real pearl — stop benchmarking your AI against a pristine expert panel no patient can access. Benchmark against the degraded, real-world baseline of care patients actually get.
🔇 Speaker Blindspot: False analogy — the AV-miles metaphor defers accountability to a benchmark nobody has defined, while the product ships today. A trust standard that can’t be stated can’t be failed.
🎙️ Turn on the Lights (IHI) — “Who Sets the Table for Quality Measurement in U.S. Health Care?” (an encore episode, re-released this week — worth it)
Dr. Michelle Schreiber, who leads quality measurement at CMS — joined by Battelle’s Brenna Rabel — says the quiet part plainly: the HbA1c >9 threshold sits where it does because reporting entities needed to score well — a negotiated political artifact, not a clinical optimum. CMS’s portfolio is shrinking from ~750 measures toward ~470, MIPS is collapsing into 27 MVPs, and 70 FHIR-specified eCQMs are live.
“If you’ve seen one electronic medical record, you’ve seen one.” — Michelle Schreiber
💡 Builder take: Treat every quality threshold as contingent config, not clinical truth — and note that roughly a third of quality-department staff time still goes to manual chart abstraction. That’s the automation surface hiding in plain sight.
🔇 Speaker Blindspot: Technological solutionism — after a masterclass on how measures get gamed, both guests wave in AI chart-reading as the fix, never acknowledging that the gaming will simply migrate into the documentation the AI reads.
What are you building this week? Email and tell me (kevin@clinicians.build) — I read every one.
— Kevin & AI